Delirium is a temporal mental disorder associated with fluctuating brain alterations that bring about emotional changes, confusion, restlessness, hallucinations, and delusions. It is also associated with difficulty paying attention, sleeping, thinking, remembering, and many more outcomes (Gorski et al., 2017). This condition only prevails briefly, usually for days or hours (Martinez et al., 2012). The most crucial worry for this condition is the time elderly patients spend in hospitals before discharge. A prolonged stay in a hospital by a patient increases treatment costs and further complications of delirium (Martinez et al., 2012). Therefore, there is a need to develop effective interventions that can prevent delirium incidence in acute hospitals. This essay provides insights and critical analysis of two interventions: the first one is the application of non-pharmacological intervention in acute hospitals, and the second one is the modified hospital elder life program (help).
The non-pharmacological intervention
This program was designed to curb the complications among old inpatients in hospitals. In Australia, this program was serviced by trained volunteers not in the medical profession (Gorski et al., 2017). Various researchers have tried to establish the length of hospital stay by applying for the multicomponent non-pharmacological program. However, they didn’t develop reliable findings to ascertain or support their evidence on LOS (Gorski et al., 2017).
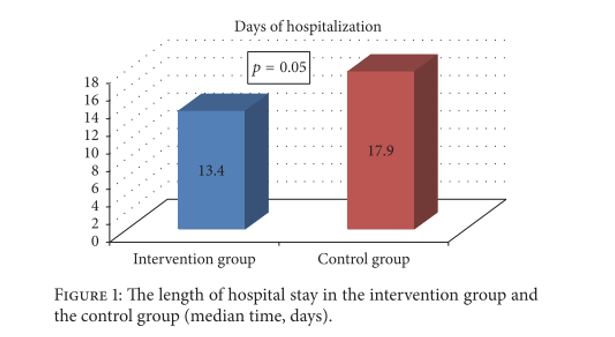
According to the research carried out by Gorski (2017), it reported the first empirical-based evidence that the application of the multicomponent non-pharmacological program reduced LOS through volunteers. According to this research, it was noted that there was a difference in statistical significance in LOS between the control group and the intervention group, as shown in Figure 1 below. This is an indication of the quality of care behind this intervention.
The volunteers in the non-pharmacological multicomponent intervention will go in pairs to visit patients purposely to reduce the burden and workload of caring. Volunteering groups must establish trust with patients to avoid doubt and allow for successful program implementation (Gorski et al., 2017). The first visit the volunteers make involves creating contact with the patients, and later on, the volunteers will engage specific patients separately daily, especially in the evening hours. The conversations between the patients and the volunteers involve discussing the patient’s needs and further sharing details on the caring aspect. In this regard, the volunteers can share their experiences and are even more encouraged to discuss them with the rest of the teams during monthly meetings (Gorski et al., 2017).
This intervention is effective on a big scale for elderly surgical patients by reducing the length of stay in the hospital’s ward. However, it is a process that requires plenty of patience to help an old individual from undergoing incidences related to delirium. Plenty of challenges accompany the individual volunteering to assist in implementation. Some of the challenges can be categorized as personal-based or ones inclined to be on the side of the patients. Personal challenges in this context can be an exhaustive activity; it requires plenty of time to spend with patients. At some point, patients may require frequent visits that might not be available.
Similar research was conducted by Martinez et al. (2012), who applied the concept of non-pharmacological intervention to elderly inpatients by using family members as volunteers to carry out the exercise to see whether the incidence of delirium could decrease. Family members were allowed to implement certain specific measures that could readily influence the growth of delirium. In this regard, they could make frequent visits, give out orientational objects, and provide support equipment, among others (Martinez et al., 2012).
The research by Martinez et al. (2012) showed a positive statistically significant difference between the controlled group and the group assigned to the program. Whereby the inpatients assigned to this program had reduced episodes associated with delirium, whereas the control group had more frequent episodes. Therefore, in this research, it can be concluded that the non-pharmacological intervention on elderly inpatients using family members as volunteers can be an effective strategy to reduce incidences of delirium (Martinez et al., 2012).
Non-pharmacological intervention is an effective strategy in both scenarios of applying non-medical volunteers and family members. However, the non-pharmacological intervention that involves family members tends to be more effective because it can reduce delirium episode’ incidences, which can consequently minimize the length of stay (LOS)
Modified Hospital Elder Life Program (mHELP)
M-HELP intervention is mainly used by older patients who are undergoing abdominal surgery and are vulnerable to delirium incidences. The program was established to reduce the length of hospital stays and the incidence of delirium. Trained nurses normally implement it. M-HELP comprises three major protocols: early mobilization, nutritional assistance, and communication orientation. Inpatients receive the mHELP treatment immediately when they enter the inpatient ward. Subsequently, after the interim has been done, the caring procedure will persist until the patient gets discharged from the hospital (Chen et al., 2017).
However, the program is accompanied by normal care that the residents offer, surgeons, physical therapists, and nurses in general surgery rooms. According to the results given by Chen and others (2017), show that the M-HELP intervention was very effective for older patients that were undergoing malignant tumor surgery. A clear reduction of delirium incidence was noted afterwards, rated at 56% reduction, and the length of hospital stay was lowered to two days. The growth of delirium is reduced and delayed for M-HELP patients (Martinez et al., 2012).
A meta-analysis done for 14 days indicated that non-pharmacologic interventions that included at least 6 components, such as hydration, vision, hearing, mobilization, and cognition, effectively minimized the delirium incidence by 44% and reduced LOS. M-HELP aims at components similar to a unique extension of applying facial exercise and nutritional assistance to facilitate efficacy on mouth swallowing that will also lead to better oral intake.
Diverting the attention of older patients to increased efficacy of swallowing, fluid repletion, and physical activity, among many other activities of a similar kind, will be of great significance in reducing LOS and incidences of delirium (Martinez et al., 2012).
Effective implementation of the M-HELP intervention requires consultations of proactive geriatrics, training members of families through sustainable educational skills, and application of software to detect symptoms of delirium incidence. The M-HELP requires daily consistency, which may, in turn, require the nurses to be acquainted with all the protocols that are under the M-HELP intervention (Martinez et al., 2012).
From the above analysis, the two interventions are important in reducing the implications that emerge from The incidence of delirium. However, one might not be as effective as the other one. Regarding this analysis, non-pharmacological multicomponent intervention is an effective program since it does not require medical experts to initiate it, unlike the Modified Hospital Elder Life Program (mHELP), which embraces the deployment of only parents and medical experts. Non-pharmacological multicomponent intervention is cost-effective since it only uses volunteers who only go for a few training skills. Besides, it is a flexible program whereby volunteers can visit the patients and share experiences.
References
Chen, C. C. H., Li, H. C., Liang, J. T., Lai, I. R., Purnomo, J. D. T., Yang, Y. T., … Inouye, S. K. (2017). Effect of a modified hospital elder life program on delirium and length of hospital stay in patients undergoing abdominal surgery: A cluster randomized clinical trial. JAMA Surgery, 152(9), 827–834. https://doi.org/10.1001/jamasurg.2017.1083
Gorski, S., Piotrowicz, K., Rewiuk, K., Halicka, M., Kalwak, W., Rybak, P., & Grodzicki, T. (2017). Nonpharmacological Interventions Targeted at Delirium Risk Factors, Delivered by Trained Volunteers (Medical and Psychology Students), Reduced Need for Antipsychotic Medications and the Length of Hospital Stay in Aged Patients Admitted to an Acute Interna. BioMed Research International, 2017. https://doi.org/10.1155/2017/1297164
Martinez, F. T., Tobar, C., Beddings, C. I., Vallejo, G., & Fuentes, P. (2012). Preventing delirium in an acute hospital using a non-pharmacological intervention. Age and Ageing, 41(5), 629–634. https://doi.org/10.1093/ageing/afs060



